
Jeff Ryckman
@jryckman3
Medical Physicist ➡️ MD | Dedicated to LR-PFS 🎯, QoL, isotoxicity ⚖️, constraints 🙅♀️, & reproducibility 📊 | Creator of @RadOncReview | #RadOncCalc
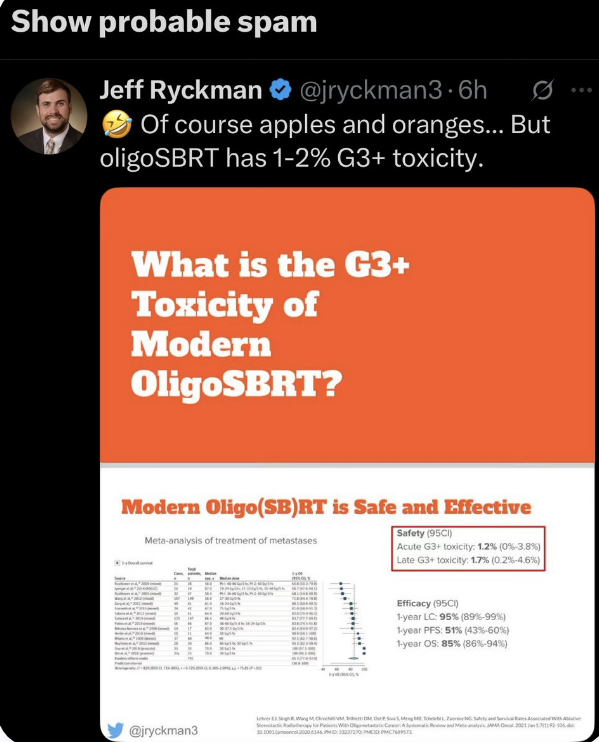
Apparently this post, which just states facts, is flagged as “Probable Spam” by @X, yet ivermectin anecdotes rack up millions of views. @elonmusk - your app is broken.
1/ Just published in @IJROBP: “Histological Classifier of Radiosensitivity to Spine SBRT.” doi.org/10.1016/j.ijro…
That's a good illustration of the issue. Even when I look back at our own protocols, there's not internal consistency sometimes. Here are the SUNSET constraints, which we pulled from other trials...in generally the shorter fractionations are allowing for higher BED (if you…
1st pt in Ireland randomised on the oligomet breast cancer TAORMINA trial in St. Luke's Hospital. Well done to all involved. Thsi trial offers pts the chance to have high dose radiation to discrete areas of cancer spread on this important trial! #breastoncology #clinicaltrials
You're totally right...one problem in RO is that dose constraints are inconsistent across protocols, especially when we compare SBRT vs. conventional. To be safe, we assumed that most of these will be stage III cases, conventionally fractionated. At least this will be a starting…
Yes, definitely. We haven't published the protocol yet, but our description of the trial from ESTRO last year is here: dropbox.com/scl/fi/9xohgt3… I'd be interested in any thoughts/feedback.
For example, let’s say the PTV includes the heart, and for the purpose of this illustration let’s say the PTV does not include a coronary artery. If planning SBRT to 54/3 or 50/5, do you limit heart D0.1cc to 30.5/3 or 37.9/5 (strict)? RTOG 0813 allowed heart Dmax of 52.5-63/5
#RealWorldData advocates facing challenges addressing sources of bias suggest causal modelling as a solution. Doesn’t work. Comparison of 19 modelling studies with #RCTs showed 42% differed in direction and 47% of confidence intervals didn’t include RCT estimate.…
Rohann Correa’s talk today at the Yonsei RO Grand Round Seminar was incredible.👍 High-level talks like this are truly rare in Korea, where geographical and language barriers remain. It was a big hit—especially inspiring for residents and students. Thanks again, @DrCorreaRO .🙏
I recently saw a patient 9 years following early-stage glottic larynx SAbR (on our original CyberKnife trial). The images below represent the typical endoscopic appearance. Our G-FORCE phase II RCT (LT-SAbR versus whole larynx) is now ~ 33% accrued! clinicaltrials.gov/study/NCT06080…
Our newest CAPRI trial, called PREVENT, is a phase II/III RCT testing high dose palliative RT for NSCLC to dose of 35/5, with esophageal sparing. 🇨🇦 We hope this will improve survival and QOL. Congrats @goodmanC_MD for getting this off the ground! ⬇️⬇️⬇️
Thrilled to activate PREVENT! This phase II/III RCT builds on the success of @DrAlexLouie's PROACTIVE trial by randomizing patients requiring palliative thoracic RT 2:1 to high-dose esophageal-sparing vs. traditional palliation to a max dose of 30 Gy in 10 equivalent
My Christie colleagues published data show its the experience of the surgeon that matters amd that complications rate not much more and OS same as with primary cystectomy
I often hear that post-TMT cystectomy is “fraught with complications even in experienced hands.” That hasn’t been my experience. With the right principles and disciplined technique, these cases can be remarkably straightforward. Maybe I’m delusional - but curious to hear what…
Thrilled to activate PREVENT! This phase II/III RCT builds on the success of @DrAlexLouie's PROACTIVE trial by randomizing patients requiring palliative thoracic RT 2:1 to high-dose esophageal-sparing vs. traditional palliation to a max dose of 30 Gy in 10 equivalent
11/14 Each year, on or around my ‘diagnosis day’ of October 17th, I try to celebrate by running the number of years it has been since my diagnosis in miles.
1/14 When I was 14 years old, soccer was everything to me. I wasn’t the best player, but I prided myself on my endurance. In the fall of 2005, I started becoming winded very easily.
9/ VCF requiring stabilization (kyphoplasty and/or surgical fusion) at 2 years: • 24 Gy in 1 fx: 11% • 30 Gy in 3 fx: 3% • 27 Gy in 3 fx: 2% (p<0.001)
8/ Key findings on LF at 2 years: • 24 Gy in 1 fx: 7% • 30 Gy in 3 fx: 11% • 27 Gy in 3 fx: 17% (p<0.001) Higher biological effective dose (BED) is associated with better local control.
7/ We compared 3 regimens: • 24 Gy in 1 fraction (fx) [n=574; 21%] • 27 Gy in 3 fx [n=1,197; 44%] • 30 Gy in 3 fx [n=931; 34%]
100% As an esophageal surgeon, I’ll be the first to confirm the potential morbidity of esophagectomy However, Do not minimize the QoL impact of preserving an obstructed, inflamed, dysfunctional esophagus!! Remember, data show post-esophagectomy QoL returns to population mean
Great to see this manuscript finally in print. Take home point - although QoL dips during the first year after esophagectomy, this metric increases and reaches the population mean by 3 years. @annalsthorsurg @YonNevo @tssmn sciencedirect.com/science/articl…