
Yannick Leyka
@yannleyka
I saw a post on LinkedIn giving advice to surgical trainees. One line really stuck with me: “Is it urgent, or is it just loud?” I’ve been using it on call today to stay focused and keep from getting overwhelmed. Simple, but its been helping so far.
A SUPERSTAR ACADEMICALLY AND CLINICALLY ✨✨✨✨✨✨✨
FCS(SA) Intermediate in the bag. It’s hard to explain how much this means to me. Not just because it’s a tough exam, but because of everything I had to push through to get here. Today, I’m standing halfway up the summit. One exam to go.
FCS(SA) Intermediate in the bag. It’s hard to explain how much this means to me. Not just because it’s a tough exam, but because of everything I had to push through to get here. Today, I’m standing halfway up the summit. One exam to go.
“Burnout is a not a badge of honor. Rest is productivity too.”
My favourite senior registrar is a consultant, FCS (SA) in the bag. I honestly couldn’t be happier.
Of all the short courses I’ve done, this was by far the best. It truly ushered me into a new stratosphere of skill and knowledge. Learning in a controlled, no-stakes environment—watching the textbook come alive before my eyes was truly a beautiful experience.
When you can’t remember the patient’s name but you’re already at the blood gas machine.
“Keep suctioning. Sister, another swab and an artery please. Call the senior. Doc, how’s the pressure? Another swab. Doc, I need you in theatre now. Sister, another swab. I see the bleeder—Vicryl please!” Anaesthesia: pulse 140, systolic 80. Did you get the bleeder? “I got it.”
I’ve got 12 patients on the emergency board and it’s only 2pm. This call has barely started.

One thing of about necrotising soft tissues infections, the smell follows you home.
My migraine triggers include lack of sleep, bright lights, fatigue, dehydration, hunger, stress, and loud noises. In other words, the standard on-call starter pack. So yes, every call shift is basically a scheduled migraine.
A call isn’t complete without a referring doctor—exaggerating symptoms to describes the patient as toxic and peritonitic, just for them to arrive relaxed, normal vitals with a marshmallow soft, non-tender abdomen, with CRP of 2, WCC of 4. I’ll never understand the reasoning here.
Almost caught up with my logbook — still about month behind but making progress. 450+ cases in 16 months is a reminder: show up, do the work, and the numbers will follow. Theatre is where the real growth happens. The nursing staff aren’t exaggerating, I really do live in theatre.
Sundays are for writing: I understand it Now by Yannick Leyka. thoughtsandprescriptions.wordpress.com/2025/04/27/i-u…

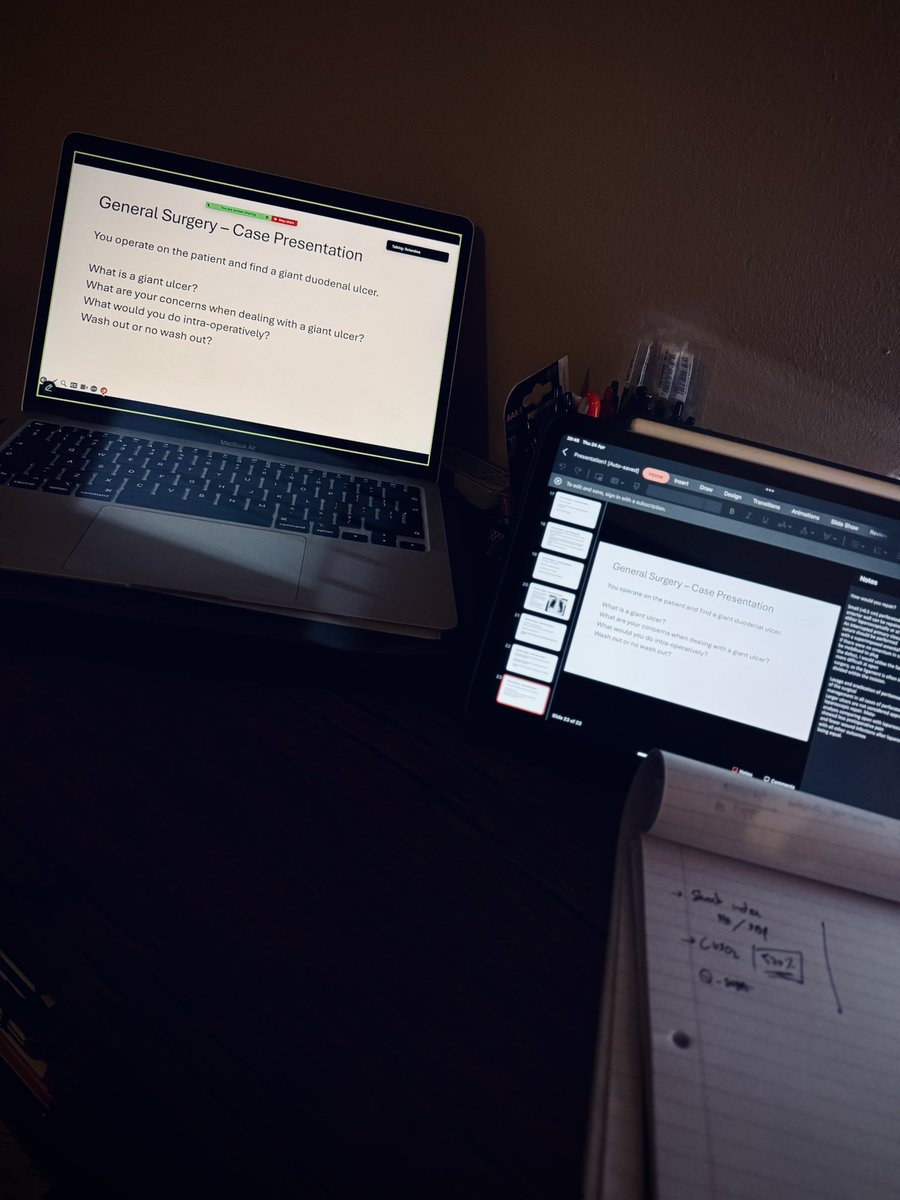
Thursday evening = study group grind. Always a blast when I’m hosting and doing the grilling — the discussions stay fire. Had a few jaw-drop moments too. Like… what do you mean your circuit relooks all perf PUDs? Definitely one of my favourite things to do.
The fact that I had a call from hell, got home in the afternoon, took an hour nap, woke up to hop onto a group study session that only just ended. Now I’ve gotta quickly do tomorrow’s M&M then study after that. My crash won’t just be glorious, it’ll be forensic case material.
Last night’s call didn’t need to go down like it did. But on the upside—managed three trauma laps, a four-quadrant sepsis, and a relook for an anastomotic leak, without needing to call the consultant out. Learned a lot, maybe grew a bit. We’re really levelling up and BECOMING.
