Austin Camp
@austincamp
Critical Care PharmD, BCCCP; Associate Professor of Pharmacy Practice; Surgical ICU
Me when someone says, “wait, you mean pharmacists work in hospitals?”
We need a head-to-head double-blinded RCT of cane sugar versus high fructose corn syrup to put this debate to rest
Great thread of some brilliant folks (not me) discussing GPC bacteremia What I gathered (basically): -Empirically likely no benefit of BL+Vanc -Vanc most common empiric monotherapy -BL > Vanc for MSSA -Cefazolin > other BLs for MSSA -As always, tailor to patient when possible!
You know what’s worse? The care plan for SAB in our area, developed by ID docs, recommends vanco AND cefazolin dual therapy pending speciation!!
The Static/Cidal letter to the editor at AAC made Google News! First time I’ve ever seen that happen to a letter to the editor—must be a ton of people reading it!
"However,the concept of static/cidal antibiotics is neither complex nor context-dependent;it is rather a myth. Regrettably,this dogma continues to be raised in modern literature despite two fundamental flaws" Honored to contribute to this important letter led by 🌟 @BradSpellberg
I can vouch that I still see this hesitancy, even from ID physicians… 😮💨 @ABsteward @BradSpellberg @DrToddLee
The reply to our letter @BradSpellberg This shocking! "indeed,not even 2 months ago we had a discussion w a Professor of Infectious Diseases about his hesitancy to treat Staphylococcal bacteremia with linezolid solely due to it being a bacteriostatic drug" journals.asm.org/doi/10.1128/aa…
Check it out! So grateful for the opportunity to collaborate on this letter. 🙏 @BradSpellberg
Static vs. cidal: it’s not complex; it’s simply incorrect @BradSpellberg @DrToddLee @ABsteward doi.org/10.1128/aac.00…
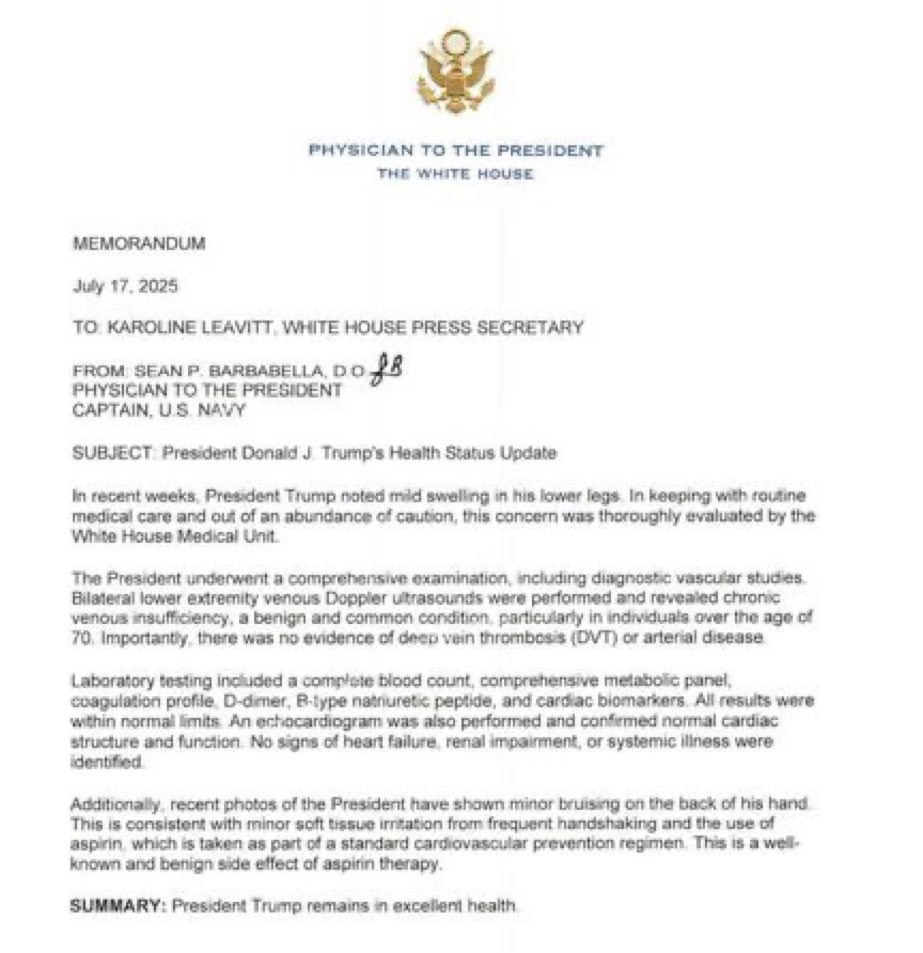
I’m more concerned about the aspirin for primary prevention in a 79-year-old. Didn’t the USPSTF recommend against that??

As an infectious diseases physician and vaccine specialist, I need to address several serious misrepresentations, baseless assertions, and factual errors in this post. 🧵
My experience working in the Ebola response on 2014 re-enforced a very different lesson than that of the COVID policy wonks, who ran Operation Warp Speed and then the Biden White House Response. That is that vaccines would never be the answer to an ongoing viral outbreak. Just…


To all the new attendings: you got this! Trust your training, but also know you will continue to learn and get better every day. More importantly, ask your pharmacists lots of questions!

Seriously, anyone know the max volume for IM and SUBQ injections??
To your knowledge/per your hospital policy, what are the max volumes for IM and SUBQ injections?
To your knowledge/per your hospital policy, what are the max volumes for IM and SUBQ injections?
I don’t know who needs to hear this, but just because a medication requires renal dose adjustment does NOT mean it is nephrotoxic!
Just because an antibiotic “covers” an organism doesn’t mean it COVERS that organism
The Pitt taught me I can get away with anything in the hospital as long as I say I learned it from a case report published in the New England Journal of Medicine