ICU OnePager
@OnePagerICU
OnePager summaries of #CriticalCare topics 1️⃣📟 | critical care education one page at a time | free & open source | #FOAMed #FOAMcc | created by @nickmmark
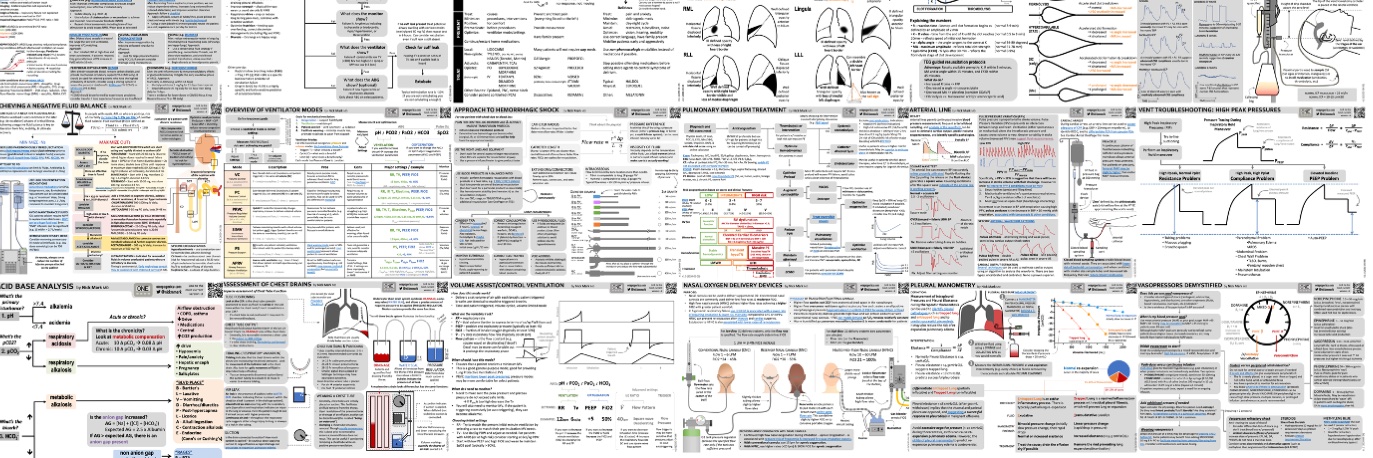
This week will be sharing some of the most popular #ICUOnePagers onepagericu.com 1️⃣ Overview of Ventilator Modes - covers all the common modes (VC, PC, PRVC, PS, APRV) & the pros/cons of each. Also covers the settings for each & how to adjust based on ABG/SpO2.

I got tired of flipping through a dozen PDFs to find the ECMO pressure/flow curve I needed. So I made an app! Choose a cannula/size & see the flow for a given pressure drop or compare multiple cannula at once. Lmk what y’all think. More cannula? onepagericu.com/ecmo-calculator
🚀 Get excited for a special year end episode talking about SPACE MEDICINE with guest astronaut Dr @shawnapandya! 🍏 podcasts.apple.com/us/podcast/cri… ✳️ open.spotify.com/episode/2magAb… 📽️ youtu.be/f0ZaOhEhYdw?si… 📑 criticalcaretime.com/episodes/40-sp…
Improved version now shows the maximum flow for a given pressure drop.
Want to learn how to: 🤖 use LLMs in medical education 🖼️ make infographics 🎧 record podcasts 📡 disseminate MedEd using social media 💰 & get paid for you MedEd work Get excited for the upcoming Digital Education & Artificial Intelligence conference! cmecatalog.hms.harvard.edu/digital-educat…
Hope you found this 🧵 useful. Let me know if you have any more suggestions for how to minimize the harms of the the #IVFluidShortage! 25/25
1️⃣6️⃣Address climate change! Ultimately we can expect more shortages & we will need far more IV fluids if we fail to address the root cause of medical supply chain disruptions: Anthropogenic climate change! I'll leave it here as this isn't my expertise... 24/
1️⃣5️⃣ Eliminate shipments to med spas providing unnecessary fluid infusions Med-spas are a poorly regulated $15b industry. Increasingly they charge $100s to provide IV fluid. This is not just medically dubious, it wastes a scarce resource. Let's stop the sale of IVF to spas! 23/
1️⃣4️⃣Allow imports from Europe To ensure quality, the FDA generally bans the import of meds manufactured outside the US. This makes sense. It would be beneficial to have a streamlined process to approve imports from trusted manufacturers in Europe. It worked with babyfood! 22/
Expanding the Strategic National Stockpile would enable it to function more like the much larger strategic petroleum reserve (SPS), not just used in crises but also acting as a "buffer" to prevent shortages of essential meds. 21/
1️⃣3️⃣ Expand the CDC's strategic national stockpile (SNS) As we saw with national shortages early in COVID, we need a larger investment in the SNS. In addition to PPE, vaccines, antibiotics, this should also include other essential meds & IV fluids. aspr.hhs.gov/SNS/Pages/Stoc… 20/
1️⃣3️⃣Get pharma to DECENTRALIZE 60% of IVF were made in ONE factory; centralized production is a big weakness. We should use incentives (tax credits, infrastructure investment, streamlined approval, etc) to encourage manufacturers to build multiple factories in different regions.
1️⃣2️⃣Hospitals need more inventory IVF are bulky & take up space. Hospitals try to be lean by minimizing inventory. But we've probably overdone it. In an era of persistent supply chain challenges, we need sufficient reserves of essential meds. This means more IVF stock. 18/
As clinicians we can do a lot to minimize the harm caused by this crisis, and potentially improve care & align with best practices. But what can we do at the system level to PREVENT crises like this from happening again? Stay tuned for 6 more things we ought to do... 17/
1️⃣1️⃣Don't use boluses to wean off pressors This strategy almost always fails; once in the deresuscitation phase almost all ICU patients are euvolemic or overloaded. Instead consider midodrine (start at a high dose) More here: onepagericu.com/blog/evidence-… podcasts.apple.com/us/podcast/7-v… 16/
1️⃣0️⃣Don't wait for central access to begin vasopressors There is ample evidence that peripheral pressors are safe and effective if done right. (adequate size/location PIV, frequent checks, protocol for extravasation, etc). I discuss this more here: podcasts.apple.com/us/podcast/6-v… 15/
9️⃣ Consider vasopressors EARLY in sepsis, instead of giving repeat boluses Early initiation of vasopressors (within the first 6 hours) after adequate fluid loading is associated with reduced mortality. annalsofintensivecare.springeropen.com/articles/10.11… 14/
8️⃣ Consider albumin in select sepsis patients Even among people who need boluses (e.g. hypotensive AND fluid responsive) is balanced crystalloid the right fluid? Not always. Consider albumin in people who may require a lot of crystalloid. pubmed.ncbi.nlm.nih.gov/37078161/ 13/
7️⃣Check fluid responsiveness before boluses Only ~50% of ICU patients benefit from boluses (the rest may be harmed). Instead of empiric fluids, we should use tests of fluid responsiveness to determine who should get fluids. See my ICUOnePager for more: onepagericu.com/fluid-responsi… 12/
(If for some reason you must use TKO be sure to use a very low rate! This is associated with similar or better outcomes.) pubmed.ncbi.nlm.nih.gov/26643858/ 11/
6️⃣No KVO/TKO "Keep vein open" or "to keep open" infusions do not improve IV patency compared to flushes. This also liberates patients from pumps, enhancing mobility & may reduce ICU LOS & duration of mechanical ventilation. pubmed.ncbi.nlm.nih.gov/33552320/ pubmed.ncbi.nlm.nih.gov/33172866/ 10/