Benjamin Besse
@BenjaminBesseMD
Medical Oncologist- Lung cancer, thymic & NUT carcinomas. Head of Clinical Research @GustaveRoussy, Head of Scientific Chairs Council @EORTC. Tweets are my own.
Morning > Afternoon for IO? Evidence is mounting—retrospective and now prospective (210 pts, randomized, PFS HR 0.42 but no PD-L1 strat). Given IO’s long half-life, maybe only the timing of the first dose matters. #ASCO2025




Debate on L1 for EGFR mut NSCLC : ‘easy osi’ then escalate to CT-ami, or use doublet upfront? Lazertinib+amivantmab likely to extend OS by ~ 1 yr vs osimertinib, but without cross over to CT-ami. Intensify only if ctEGFR not cleared after 4w of osi? #ELCC25




ICB or chemo-ICB in PD-L1≥50% advanced NSCLC? Metabolic tumor volume (tMTV) assessed by 18F FDG petscan can guide you. High tMTV lesions might have a different biology and be better candidate to chemo-ICB. @FilippoDallOlio aacrjournals.org/clincancerres/…
NUT Carcinoma is an ultra-rare entity with a NUTM1 fusion, diagnosed by a simple IHC NUT+ (can look like a squamous lung cancer in a never smoker pt). Previously known as midline carcinoma, its prognosis is extremely poor. Lurbinectedin appears promising! annalsofoncology.org/article/S0923-…
YES! De-escalation trials matter and should be much more supported by payers! Very preliminary results from the Dutch non inferiority trial DEDICATION-1 are reassuring. In France, the PULSE trial has the same hypothesis, opens soon in Belgium, Spain, Estonia and Greece! #ESMO24




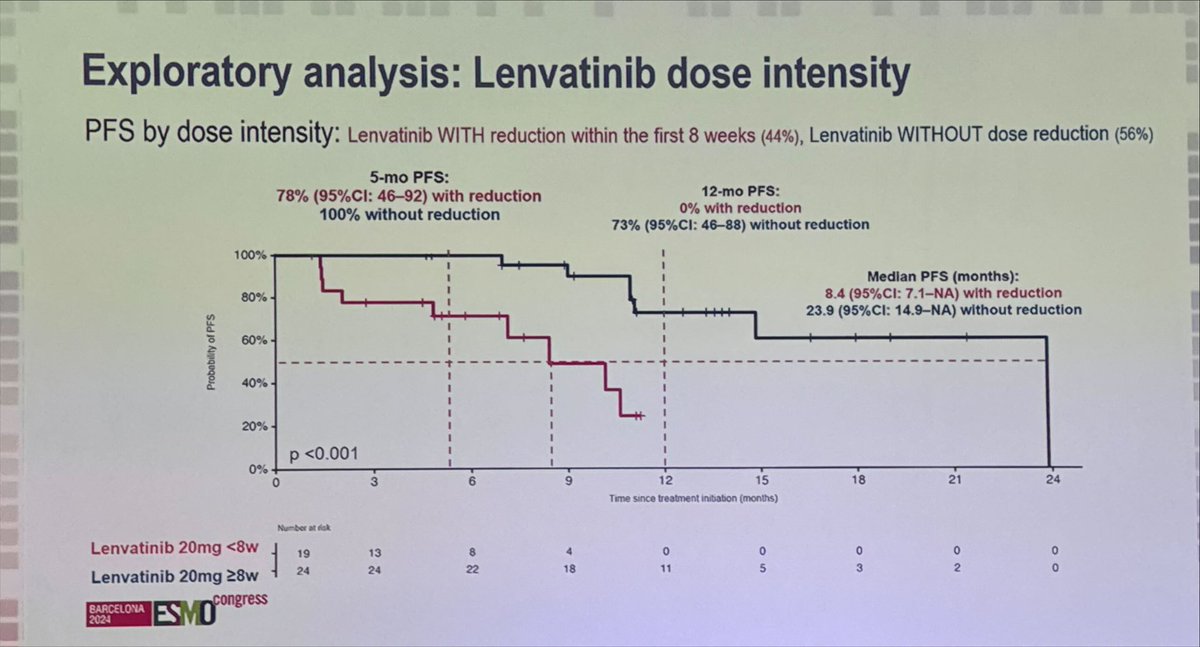
Impressive benefit for Lenvatinib-Pembrolizumab in pts with thymic carcinoma and B3 thymoma. ORR 23.3% and mPFS 14.9m are unexpected in 2nd line or more. Lenvatinib dose matters in a subgroup analysis. Congratulations @JordiRemon #ESMO24



Adjuvant Durvalumab after resection of stage IB~IIIA NSCLC does not improve DFS. No predictive effect of PD-L1 expression as in KN-091/PEARLS (adj pembro): Biology of micrometastatic disease differs from matched primary tumor? Confirms that neoadjuvant is the way to go. #ESMO24




1st phase III trial of an ADC vs docetaxel in a biomarker selected population Tusamitamab Ravtansine targets CEACAM5, overexpressed in 25% of non sq NSCLC CARMEN LC03 did not meet the primary endpoints PFS and OS. #WCLC24




Stop pembro after 2 years? In 43,359 pts that received up-front pembrolizumab for an advanced NSCLC, continuation beyond 2 years was not associated with better OS than a fixed 2-year treatment, HR = 0.97 [0.75–1.26] p = 0.95. @arousseaumd sciencedirect.com/science/articl…
In resected EGFR mut NSCLC after chemo 6 mo vs 12 mo icotinib (1st G EGFR TKI) similar DFS and OS despite only 70% completed txt. Adj OSI x 3y: 4y DFS 73% 5yOS 88%. Data in line with shorter treatment and with 1st G TKI ➡️We should explore descalating txt in this setting #ASCO24
Another promising B7H3 ADC in pts with Small Cell Lung Cancer. « SuperTopoi » payload. DAR=4. Very early data. No ILD. Unconfirmed ORR 61.3%. #ASCO24


LIFETIME osimertinib after a treatment with curative intent? In pts with EGFRmut stage III NSCLC, chemo-radiotherapy can CURE pts. Were pts in LAURA properly staged by petscan/brain RMI? Why not using MRD to select patient? Strong concerns when OS is not positive. #ASCO24




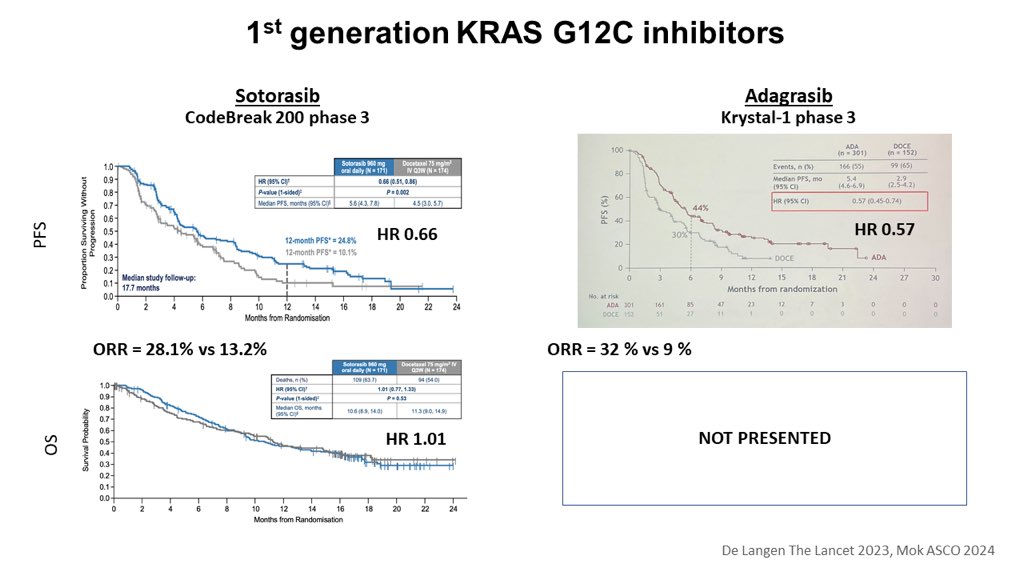
1st generation KRAS inhibitors: a piece of the puzzle is still missing. #ASCO24 Hope it will be enough to convince refractory HTAs to refund the drug! @KRASKickers
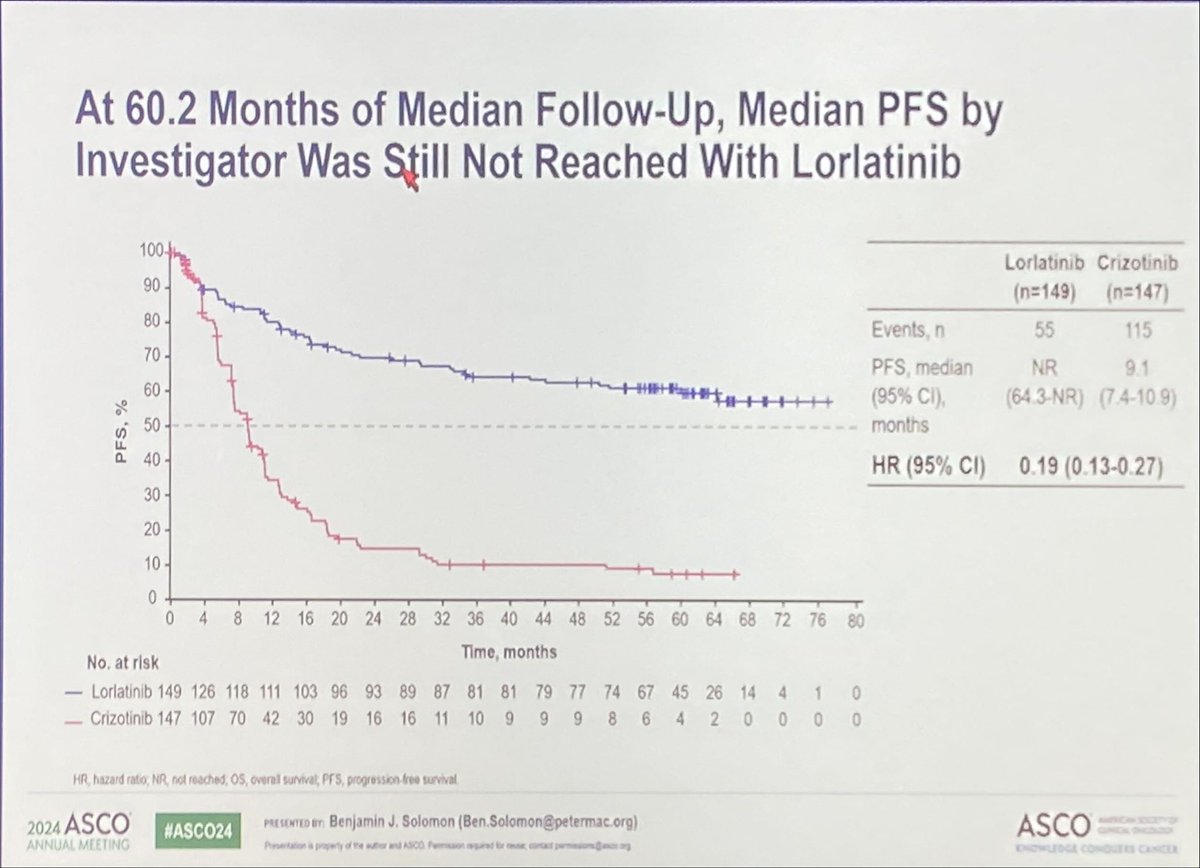
Lorlatinib PFS is impressive with an HR 0.19 over crizotinib. But why after 5 yrs FU can’t we see the OS curves and the cross over rate? Even if the number of events is not reached, that would help us to select our first line treatment. @ALKPositiveinc #ASCO24

For pts w EGFRm with Osi-Progression NSCLC not homogeneous benefit in PFS with🩸antiangiogenic + io+CT vs CT and no mature OS benefit Ph 3 HARMONI-3 trial (ivonescimab (bispecific VEGF/PD1 Ab)+ CT vs CT is pending. Data in Chinese pts looks similar to previous (HARMONI-A) #ASCO24
Important and completely counter intuitive study ! The NGR-LU002 stydy shows that the irradiation of all sites (primary+mets) after induction chemo or chemo-IO does not increase survival compared to the standard maintenance treatment. « Le mieux est l’ennemi du bien » #ASCO24



S/C route is the way to go for amivantamab! Paloma 3 trial shows similar PK of S/C vs IV with potentially better survival. Dose intensity & toxicities seem similar (but for Infusion relation reaction). Are blocking ADAs (anti drug antibodies) more frequent with IV vs S/C? #ASCO24




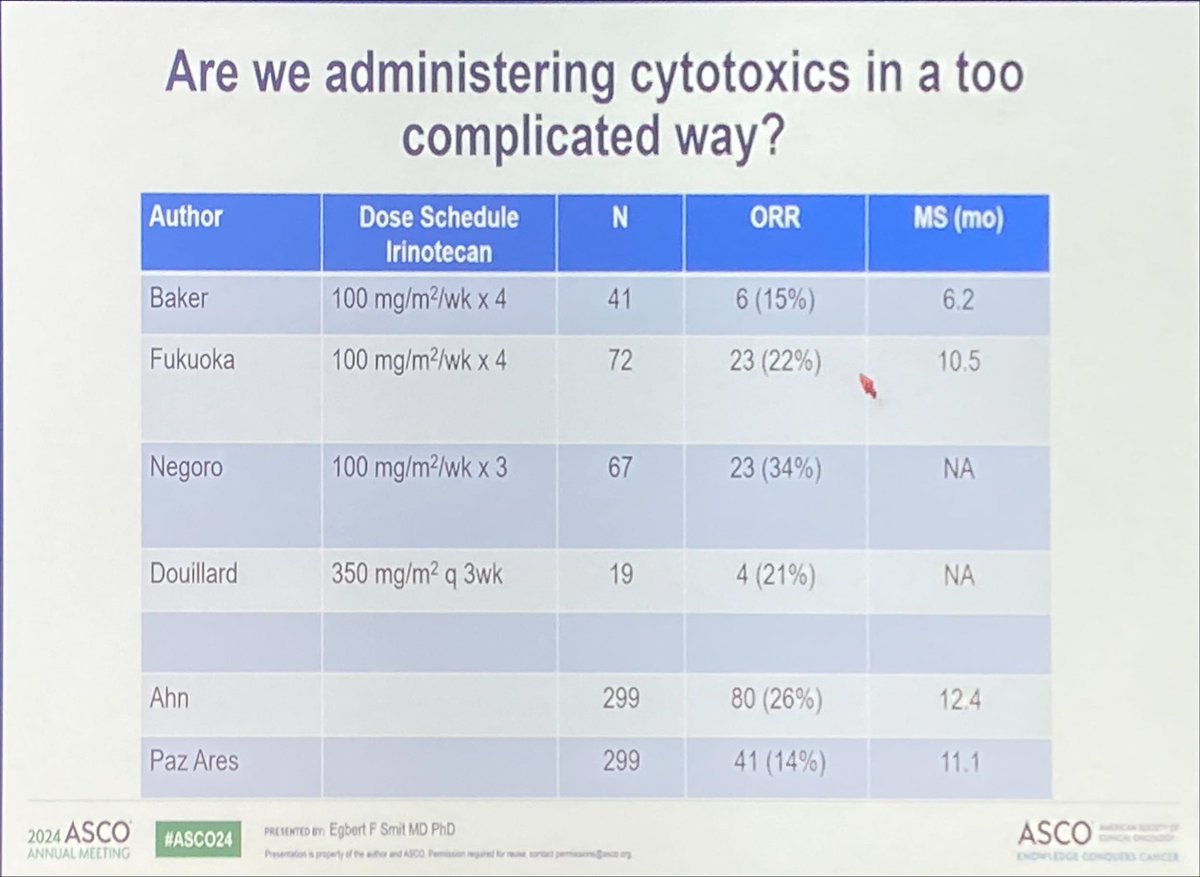
Pr @SmitEgbert elegantly suggests that TROP-2 ADCs with a topo-1 inhibitor payload (deruxtecan, govitecan…) are not better that old fashioned topo-1 inhibitors such as irinotecan or topotecan.
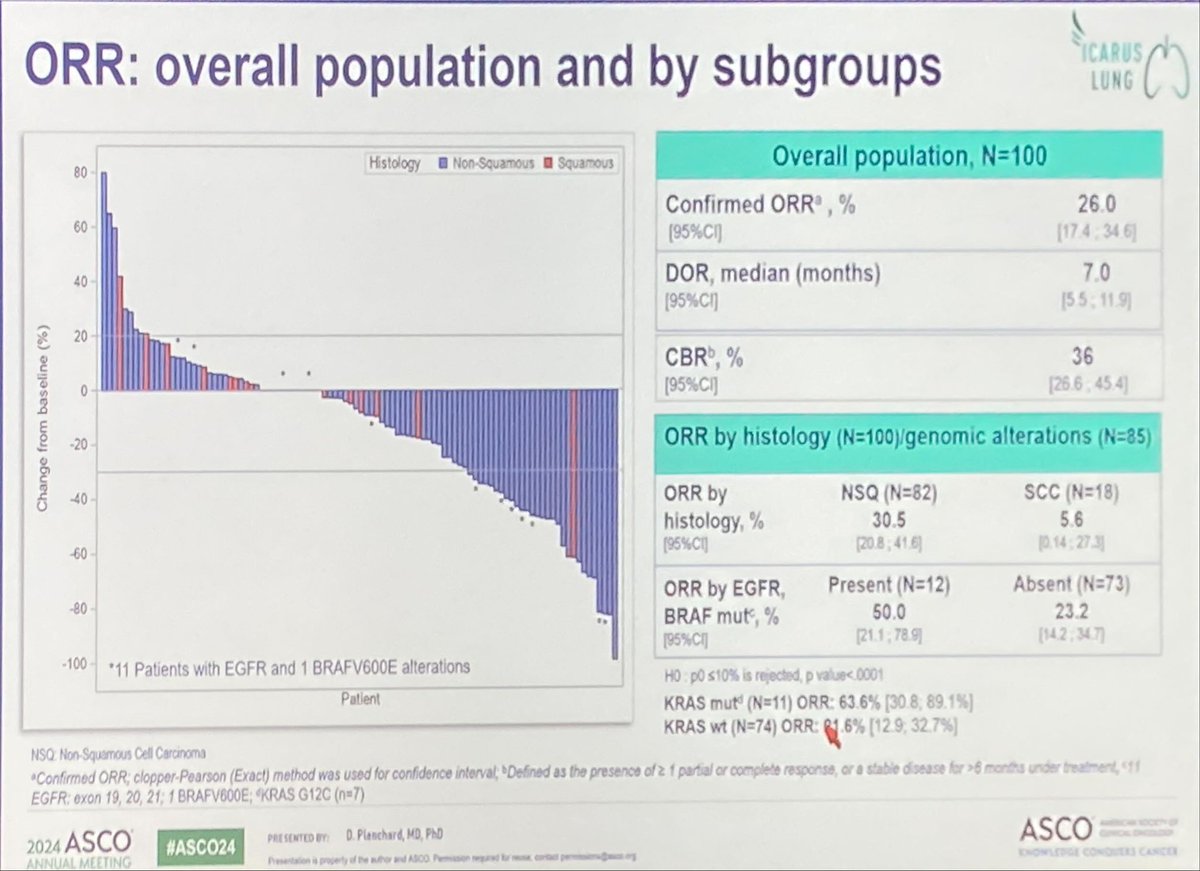
Two new studies support the hypothesis that pts with EGFR mutated NSCLC are the best population for TROP-2 ADCs: EVOKE-01 (EGFR is in the ‘AGA’ subgroup in the forest plot) and ICARUS-LUNG. @dplanchard @EGFRResisters #ASCO24